Sabrina Mukhtar, MD, MPH, Director of the Dry Eye Center of Excellence at the UPMC Vision Institute, was excited to share the work they are doing in the Eye & Ear Foundation’s October 9th webinar, “Personalized Approach to Dry Eye Care.” Her goal was to show why the Vision Institute is different when it comes to treating dry eye and personalizing that approach for patients.
What is Dry Eye Disease?
A 2007 Report of the Definition and Classification Subcommittee of the International Dry Eye Workshop defined the condition as, “a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface.”
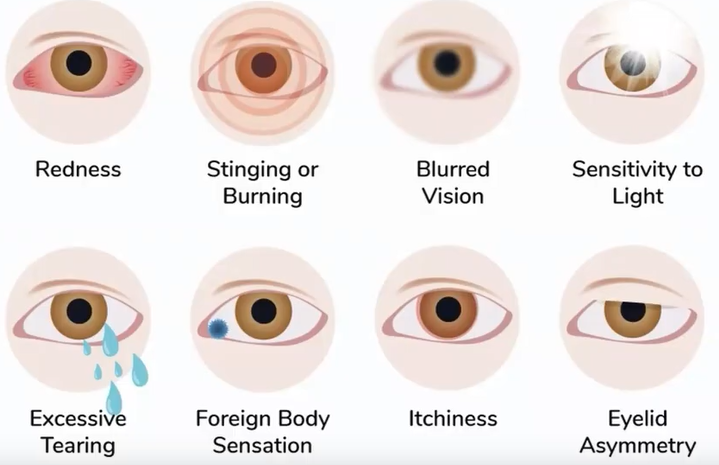
Symptoms include redness, stinging or burning, blurred vision, sensitivity to light, excessive tearing, foreign body sensation, itchiness, and eyelid asymmetry.
At least 30 million people have dry eye disease, and its prevalence is increasing, with a proven impact on quality of life. This condition is one of the most common problems affecting the general population, with prevalence ranging from 7.4% to 33.7%. Its impact on quality of life is comparable to dialysis and angina, and it is the number one ocular cause of depression. “This is very challenging because a lot of our anti-depressant medications cause dry eye as well,” Dr. Mukhtar said.
Dry Eye Causes
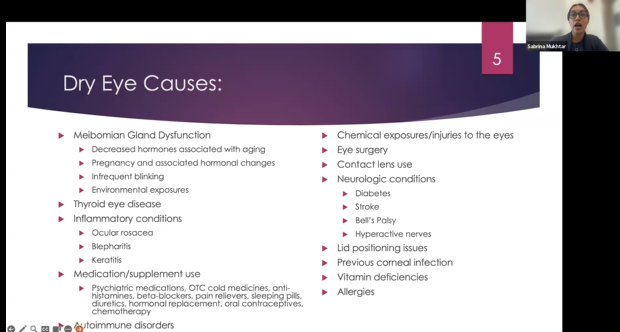
“Our goal is really to try and find the underlying cause of your dry eye disease so we can better target our therapies and come up with a great recipe for you to have success in treatment,” Dr. Mukhtar said.
Dry eye disease is very complex and highly rooted in inflammation and immunology, Dr. Mukhtar added. Having people who really understand that is critically important when treating the disease. The Center is doing a lot of great research with basic science colleagues to try and better understand inflammatory causes and the different inflammatory cycles of the disease.
Who are We?
Dr. Mukhtar praised the staff, saying, “We can’t do this without them; it’s really important to elevate them because they are doing a lot of the work. We’re a small but lean program, and very efficient, and have people who truly care about the patients.”
In the photo on the left, Tammy in the center helps patients get ready for their visit. Kristen and Terry help with testing and different therapies. Karen is the pod coordinator and helps get different procedures scheduled. The nurses, Melanie, Kathy, Savannah, and Tammy (not pictured) help with the serum tears.
“I really love that this cohort of dedicated staff really try to make this one-stop shopping for you,” Dr. Mukhtar said. “We’re able to provide a very in-depth and comprehensive approach to treating your dry eye disease.”
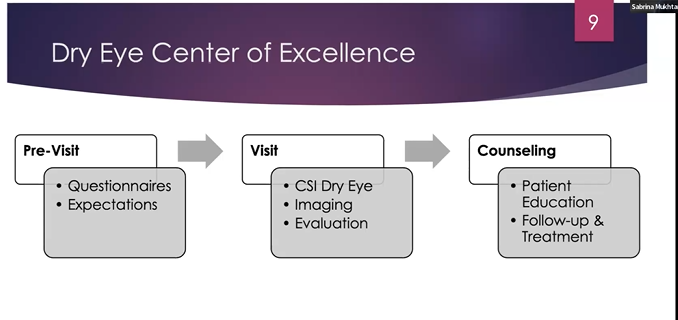
CSI Dry Eye
The Center only sees patients in one snapshot of time, but dry eye affects patients day in and out, so prior to the visit, patients receive extensive questionnaires. This is through CSI Dry Eye, a program that has revolutionized dry eye care. It is a secure machine-based learning program that delves into the different causes of dry eye disease, developed by Dr. Ahmend Al-Ghoul, a former cornea fellow at UPMC. His goal was to create something more objective, an algorithm for patients so there is some consistency.
The detailed questions go through a lot of demographic information, lifestyle, previous medications, dietary habits, etc. The technology then analyzes all that information to provide some mimickers of dry eye or things that might be contributing to it. People in Europe, all over the U.S., and thought leaders are using this program to better help characterize patients with dry eye disease.
According to Dr. Mukhtar, patients love this program; they love knowing why they might have dry eye and are then more motivated to do what they are being asked to do. “There is a little bit of understanding and acceptance, like, well, I can’t change my non-modifiable risk factors, but let’s work on the things that I can change,” she said.
The technology also looks at different questionnaires that have been validated in the literature to give more objective ratings of dry eye disease. Progress can be tracked over time like a report card, which patients also like. Patients feel better but then when they see their scores improving, they feel like they are moving towards a goal, which is “rewarding and wonderful,” Dr. Mukhtar said.
Dry Eye Imaging
One thing that sets the clinic apart is it does a lot of advanced imaging. When patients come in, it is a long visit that may take up to two hours, but they are thoroughly examined. Myibography – technology that takes images of the oil glands – along with imaging the quality of the tear film and quantifying blinking dynamics (which is extremely hard to test) gives some indices of why a patient has dry eye.
There is imaging that looks at the cornea structure and can quantify changes in the ocular surface on a very granular level. Lots of literature supports the idea that controlling dry eye disease improves patient outcomes with cataract surgery.
Sampling the tear film measures the inflammation level, called a tear film osmolarity. Dr. Mukhtar uses this on the first visit. Coche bonet checks cornea sensation. Nerves are very important in the ocular surface, and the cornea has the greatest number of nerves per surface area. “We want to know so we can protect ourselves, but certain systemic conditions can definitely affect the nerves, and there is a symbiosis between the nerves and the ocular surface and inflammatory mediators,” Dr. Mukhtar said. “We’ve found that the incidence of decreased sensation on the surface through doing this coche bonet on everybody is prevalent in patients with dry eye disease as well.”
The Visit
During the visit, the questionnaires are reviewed, testing is done, there is a slit lamp examination, and the provider talks to the patient. Together, they develop a customized regimen tailored to address the underlying cause of disease. The Center has a holistic approach to treatment and communicates with other health care providers to address underlying medical issues contributing to ocular surface disease.
Treatment Options
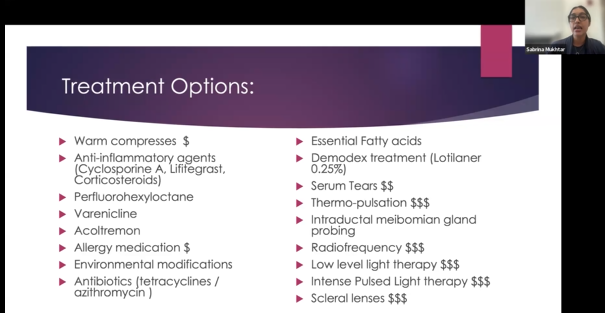
Treatment options have exploded in the last 5-10 years. The main course of treatment used to be prescribing mild artificial tears, but then providers realized the underlying cause needed to be targeted.
Allergy medications are widely used in the practice. We all have microorganisms that live on our lashes, Dr. Mukhtar said, and one is called demodex. Now there is an exciting medication called Lotilaner that has revolutionized treatment.
Serum tears are made from your own blood. Blood is drawn, the red stuff is spun out, and the plasma is used to make tears. A nurse will come up to the third floor and draw blood while patients are getting worked up. By the time the visit is done, the serum tears are delivered, which is amazing in terms of access and convenience.
Unfortunately, coverage for a lot of dry eye therapies is challenging as insurance has yet to catch up. There are out of pocket procedures offered in the clinic. Dr. Marissa Heary – who is optometry trained and did her residency and fellowship at UPMC – offers scleral lenses. These are hard lenses that go on the ocular surface and almost creates this prosthetic surface so the fluid stays on the eye. “Our patients feel so lucky to have her as part of our team because it’s something she can offer that a lot of other places may not,” Dr. Mukhtar said.
Dr. Mukhtar treats a lot of lid disease; ocular rosacea can affect the eyelids, for example. Low level light therapy has exploded in the last few years; it stimulates the mitochondria to function better in the cells, allowing the oil glands to pump better. It is supposed to decrease inflammation as well and is used for patients who have nerve issues with very positive results. This is something Dr. Mukhtar is looking to study on a larger scale, as this would be very promising for patients with fibromyalgia or herpes in the eye.
Dr. Mukhtar does a lot of intense pulse light therapy, targeting inflammatory vessels or blood vessels that are along the lid margin due to inflammation or ocular rosacea. Inflammatory mediators are brought to the surface of the eye, causing backup of the oil glands, which causes more inflammation – a vicious cycle. A lot of the typical medications put on the eye do not address the underlying cause, just the downstream inflammation. This therapy, however, targets the underlying cause. Patients do very well with it because it is not offered to everybody, only to patients who should really benefit. The lids are cleaned too.
The Vision Institute Experience
The Vision Institute offers one-stop care:
- Serum tears on site
- Co-management with optometry for specialty lenses
- Coordination with other subspecialities (oncology, rheumatology (Sjogrens clinic), dermatology, neurology)
- Active clinical trials
- Active studies – integrative medicine
- Equity partnerships to provide equal access to all
- Eye & Ear Foundation
- Donations
- Veterans Hospital
The Center also frequently collaborates with industry. Currently, the Center is partnering with Carnegie Mellon University on a study looking at the effect of mindfulness meditation in treating dry eye disease following an objective metric. Specifically, they are looking at how warm compresses affect patients with glaucoma to make sure people’s eye pressure is not being raised. There are a lot of collaborations with other countries as well.
Patients are happy to participate in research and want to help those who follow. Patients will also tell the clinic about a certain doctor they love, like a rheumatologist. Dr. Mukhtar has a little sheet of patient-suggested products as well, like mascara, etc., that she shares with patients. She has some very generous patients who have donated to help other patients who may not be able to afford some treatments. She referenced a very innovative idea she is hoping to carry out to provide more equitable care for patients and is working with UPMC finance to try to make it happen.
“Time and time again, our patients talk about how wonderful our staff is, how people really care, and how people are listening to them,” Dr. Mukhtar said. “IPL has been a game changer in our practice. We are impacting patients’ quality of life so that dry eyes are not the only thing they think about.”