“Management of Facial Trauma,” the Eye & Ear Foundation’s February 27th webinar, is a topic that makes up a large part of Christina M. Yver’s practice. The Division Chief of Facial Plastic & Reconstructive Surgery and Director of the UPMC Facial Nerve Center said it is a very satisfying aspect of her practice that keeps her busy and on her toes. “I think it’s relevant to a lot of patients,” she added.
Epidemiology of Facial Trauma
Facial injuries represent roughly 5-15% of all trauma presentations. Males are disproportionately affected, typically accounting for 70-80% of all cases. Peak incidence occurs in young adults between the ages of 20-40.
Pittsburgh has two Level One Trauma Centers: Presbyterian and Mercy. They receive referrals and transfers from all over the region, from Western PA to W VA to Eastern OH.
Certain mechanisms like falls are seen more commonly in the elderly and young children, making it a pretty heterogenous patient population.
What falls under the umbrella of facial trauma? Generally, talking about fractures of the bony facial skeleton. However, facial trauma also encompasses orbital trauma and we often co-manage those with our ophthalmology colleagues.
Types of Facial Trauma
“What falls under the umbrella of facial trauma?” asked Dr. Yver. Generally, this term refers to fractures of the bony facial skeleton. However, facial trauma also encompasses orbital trauma, which is often co-managed with ophthalmology colleagues.
Types of facial trauma:
- Mandible fracture (jawbone)
- Midface fracture
- Nasal trauma
- Orbital trauma (bony orbit or eyeball)
- Dental trauma
- Penetrating soft tissue injury
- Ballistic trauma (high velocity, a lot of soft tissue and bony destruction)
Mandible Fractures
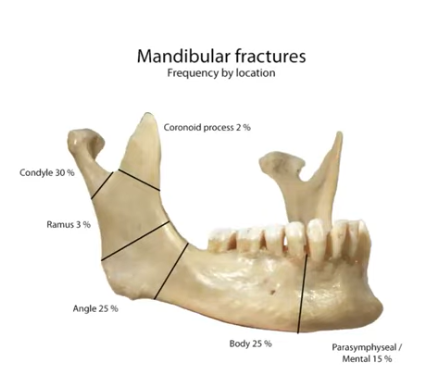
Mandible fractures are one of the most common types of facial injury seen. The most common etiologies are sports, motor vehicle accidents, assault, and falls. Falls are pretty common, especially in winter.
Common physical exam findings include bruising, fractured teeth, bony step offs, mobility of the mandible, numbness, and malocclusion. Malocclusion is a big one. It means the teeth are not coming together properly; patients may complain their bite is off or they are not able to bring their teeth together in the way they are used to).
If untreated, mandible fractures can lead to chronic malocclusion, trismus (inability to open the mouth), malunion (when the fracture never quite heals properly or the bone in that area gets chronically infected and starts to break down), and chronic pain or cosmetic deformity.
When a patient arrives at the ED, if there is any concern, they will get imaging – typically a CT scan. If this demonstrates a mandible fracture, they are evaluated by the on call facial trauma team. In the Department of Otolaryngology- Head & Neck Surgery, facial trauma call is shared with oral surgeons and plastic surgeons. If facial plastics is on call, typically one of the residents will assess the patient in the ER, determine the nature of the fracture, and usually make a preliminary call on whether that fracture is operative.
If it is operative, it needs to be addressed typically within 14 days or as soon as possible.
Mandible fractures can be tricky. “You have several strong muscles called the muscles of mastication that allow you to chew, bite down, and close your jaw,” Dr. Yver explained. “These muscles subject the various segments of the mandible to these really strong tensile forces. For this reason, if you have a fracture line, even if it is a small fracture or non-displaced, the two fracture segments can grind against each other long term, which makes it impossible for the fracture to heal.”
Often, even a small non-displaced fracture – especially if it is up in the front of the mandible – is usually operative because everything has to be immobilized to give the bone a chance to heal. That being said, there are mandible fractures that can be treated:
- Observation (no chew diet x 6 weeks) – no surgery
- Closed reduction/maxillomandibular fixation (MMF) – wire the jaw shut
- Open reduction and internal fixation – most common, make incisions, directly access the fracture by exposing it, put into proper alignment, put plates on to hold it in place
Maxillomandibular Fixation (MMF)
The important part of MMF is that you want the teeth to come together perfectly when you let the fracture heal. There are different ways to wire a patient shut:
- Arch bars – the traditional way; heavy metal bars secured to the teeth with wire, additional wires used to secure the upper teeth to the lower teeth. They’re strong, reliable, and can be left on for up to six weeks
- Advantages: Can serve as a tension band
- Disadvantages: Time consuming to apply (can take up to 45 mins; patients don’t love them)
- Wave (IMF system) – Put very small screws into the gums and wire the patient shut that way
- Advantages: Quicker to apply
- Disadvantage: Can be problematic when accessing fracture; does not serve as a tension band
- Traditional IMF screws – Isolated screws, quick and dirty wiring shut – fine if only going to wire them shut in the OR to put the plates on but would not want to leave someone like that long-term because it is not quite stable enough
- Advantages: Quick, good for posterior fractures
- Disadvantages: Not for long-term MMF; can be in the way for anterior fracture access
Pearls for Mandible Plating
- Nasal intubation (cannot put breathing tube in mouth)
- Expose and mobilize all fractures
- Trans-oral incisions (most common, make incisions inside the mouth)
- Trans-cervical incisions (external incision, dissect down onto the jawbone; have to be really careful that you are not injuring any branches of the facial nerve in that area; also a lot of arteries and veins that you have to mobilize and work around)
- Place in MMF (crucial, because you have to establish their normal bite and normal occlusion before you put plates on)
- Start by plating anterior and then work posterior
- Release from MMF and check occlusion (cut wires and make sure they are able to reestablish bite on their own)
- Close
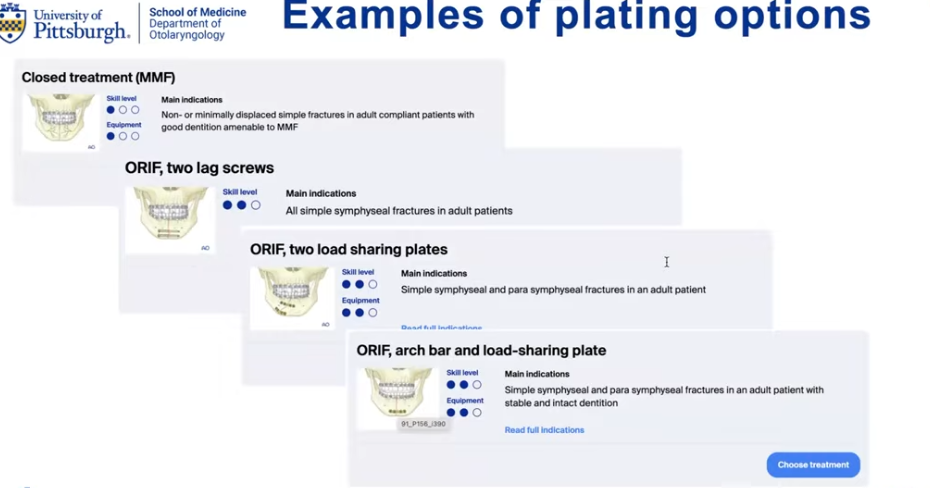
There is not a lot of nuance with how to manage fractures and put the plates on, Dr. Yver said. An organization called AO provides guidance for a lot of bony trauma. AO works with orthopedic surgeons and neurosurgeons. The website has a section on craniofacial trauma, so surgeons can use this free resource to look up any type of fracture or fracture pattern to get suggestions on appropriate ways to manage. Ultimately it is up to the surgeon’s discretion, as every surgeon has their own preference. A lot of judgment goes into each individual fracture. The following case example illustrates this point.
Case Example: Displaced Symphyseal Fracture and Right Condylar Fracture
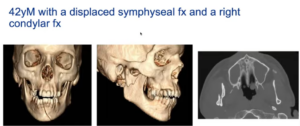
A 42-year-old male presented with facial trauma after a domestic violence – one up front, going through the front of his jaw, and one further back through the neck of the condylar. The latter can cause a height discrepancy when you bite down where there is an open bite on one side because of the loss of mandible height on the other side.
Patient specific factors have to be taken into account when coming up with a treatment plan. Generally, when Dr. Yver sees fractures like this, she might plate the anterior fracture but because the condylar fracture is technically challenging to plate, she treats it conservatively by leaving the patient in MMF for two weeks after before graduating the patient to elastics without putting in a plate.
The problem with this patient was that he was brought in by police and being incarcerated after his discharge. You can’t send someone to jail with a jaw wired shut, so his treatment had to be personalized. Dr. Yver put a plate on the condylar fracture, which involved making a separate incision in front of the ear. This meant dissecting through an anatomically complex area with big branches of the facial nerve riding over it. A nerve stimulator has to be used to identify them, work around them, and add a plate. There is not a lot of access to reduce and plate, which mitigates the need for MMF postoperatively.
The patient woke up with good facial function and perfect occlusion. Everything went really well and he was discharged. “Unfortunately, I never got to see him again,” Dr. Yver said, “which is fortunately very common in this patient population. From my standpoint, I assume no news is good news or else they would know where to find me.”
Midface Fractures
Midface fractures are a whole different ballgame. The midface is not subject to the same muscles of mastication as the mandible and occlusion is less of an issue. But it is an extremely important region cosmetically, so even minor fractures can lead to long-term changes both in appearance and contour deformities. “We do take this area very seriously,” Dr. Yver said.
Common midface fracture complexes (ZMC fracture, zygomatic arch fracture, NOE fracture, Lefort fracture) tend to follow certain patterns of injury and have specific terminology. They are typically treated non-operatively, unless there is significant displacement on imaging, a perceptible full cosmetic deformity, or severe trismus (controversial). If an operation is needed, it is typically treated with ORIF or closed reduction (zygomatic arch fractures).
Surgical Approaches to the Midface
The tricky part of midface fractures is figuring out how to access the fracture, since it is a very cosmetic area – the middle of the face. “You don’t want to make an incision wherever and leave an unsightly scar,” Dr. Yver said.
Surgeons take advantage of locations where they can put a cosmetic incision that will turn into an imperceptible scar. For fractures lower on the midface, they might make the incisions in the mouth – in the upper lip – so there is nothing external.
Surgical approaches:
- Vestibular (gingivobuccal)
- Upper blepharoplasty (incision in the crow’s feet to access fractures of the lateral orbital rim)
- Coronal (advanced approaches like this and lynch, midface degloving)
- Lynch incision
- Midface degloving
- Subtarsal
- Transconjunctival (incision on the inside of the lower eyelid)
- Direct
A lot of facial trauma is mastering these incisions and approaches.
Case Example: ZMC Fracture
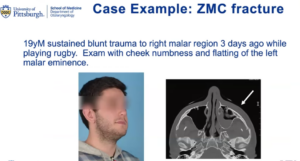
A 19-year-old male sustained blunt trauma to the left malar region three days ago while playing rugby. He mentioned cheek numbness, and upon examination, Dr. Yver noticed flatting of the left malar eminence, or loss of projection of the midface. A ZMC fracture is a fracture complex of this kind of malar region. The patient’s was depressed inward by several millimeters.
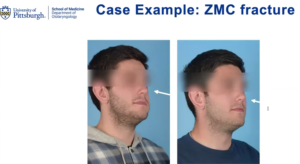
Dr. Yver called this an interesting case because it was one simple displaced segment. She was able to access it through a small incision on the inside of his upper lip. She lifted the whole thing up and popped it back into its proper position with just one mini plate to hold it in.
Post-operatively, the patient has a nice restoration of his midface contour with no external incision. “He healed up beautifully from that,” Dr. Yver said.
Case Example: Zygomatic Arch Fracture
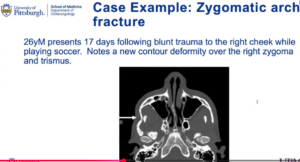
A 26-year-old male presented 17 days following blunt trauma to the right cheek while playing soccer. He had a dent in his cheekbone – a visible contour deformity. He had an isolated zygomatic arch fracture. With this, a plate is not needed; a closed reduction where it is popped into place and then left to heal. The tricky part for this kind of fracture is getting the access; there are several approaches.
Approaches to the Zygomatic Arch
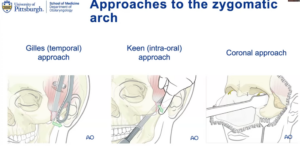
Gilles (temporal) approach – An external incision made further up in the hair to camouflage the scar. The surgeon has to get in the proper plane avoiding some of the branches of the facial nerve. Then they get an elevator under the cheekbone and reduce that depressed fragment back up to restore the contour.
Keen (intra-oral) approach – Dr. Yver personally likes this approach, where you kind of come down from below. It is the same idea as above where you get your instrument or elevator under the cheekbone and pop it back up.
Coronal approach – If the fracture needs plates, this is the way to do it.
Fortunately, in the patient’s case, they were able to do a small intra-oral incision. Dr. Yver was able to get under the fracture, pop it up, and restore the contour. “Sadly, this was another patient I didn’t get a chance to meet again,” she said, “but I’m sure he’s doing well because he had a beautiful reduction.”
Orbital Floor Fractures
ENTs manage these all the time, often in collaboration with their ophthalmology colleagues, but it presents a whole new set of challenges.

This fracture is very common, and is often called a blowout fracture, when a direct impact to the eye causes a sudden pressure increase in the orbit, which drives the thin orbital floor down into the sinus cavity below. Because of the eye proximity to the fracture, symptoms include double vision, a sunken-appearing eye, restricted eye movements, and cheek numbness. It can result from an assault, punch, sports injury, fall, or motor vehicle accident.
Fortunately, not all orbital floor fractures require surgery. Management depends on its size and what the patient’s associated symptoms are. “We typically get input from ophthalmology early when deciding whether to intervene,” Dr. Yver said.
Orbital Floor Fractures: Indications for Repair
Indications for acute repair:
- Bradycardia (oculo-cardiac reflex) – very rare cases, heart rate goes down
- Limited supraduction of the eye (indicative of inferior rectus entrapment) – muscles that move eyeball around can get stuck in that fracture line. If there is evidence that these muscles are entrapped, it is important to intervene ASAP to avoid any long-term damage
Indications for delayed repair:
- Persistent diplopia once edema improves
- Enophthalmos > 2 mm
- Malposition of the globe
- Orbital floor defect > 50%
- Associated significant facial fractures
Dr. Yver is pretty conservative about plating orbital floor fractures because a lot of these patients do well without surgery, and it is a high-risk area. If there is poor surgical technique or plate placement, issues like muscle entrapment can arise just from the repair. Another issue is when the lower eyelid is malpositioned and scar bands form in the eyelid. If it is a significant defect, surgical intervention should be considered.
Case Example: Orbital Floor Fracture
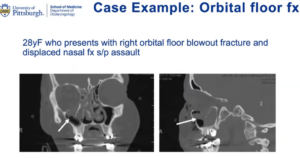
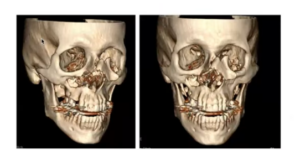
A 28-year-old female victim of assault presented with a right orbital floor blowout fracture and displaced nasal fracture. The fracture encompassed a large portion of the orbital floor. Dr. Yver was worried she would have a long-term issue, with the fracture affecting her vision or the eye sinking down into the orbit. She was taken to the OR.
Generally, when surgeons intervene in cases like this, they repair them by inserting a plate into the orbital floor to hold up the orbital contents. These plates can be made of titanium, which is Dr. Yver’s preference. They can also use plates made of other biocompatible synthetic materials like porous polyethylene.
Most commonly, the way they access the orbital floor is through a trans-conjunctal incision. This is made in the conjunctiva of the lower eyelid. The lower eyelid is pulled down, and an incision is made on the inside of the eyelid. Meticulous dissection is done down to the orbital floor, the contents are lifted off the bony defect, and a plate is slid in.
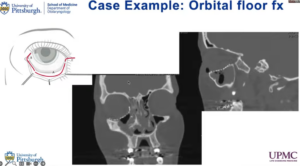
The challenging part is to make sure the plate is sitting perfectly after surgery. “A lot of us will get imaging postoperatively to confirm the plate is sitting perfectly,” Dr. Yver said. “This one is.”
Dr. Yver is proud of this image and said you can see that posteriorly all the way far back, the plate is resting on the posterior ledge. This is exactly what you want to see. The trickiest part about plating these is probably getting the plate to sit perfectly all the way back.
Nasal Trauma
Dr. Yver sees a lot of nasal trauma in her practice because she does a lot of nasal surgery. Nasal fractures are the most common type of facial fracture, making up ~50% of all facial fractures. This does not involve just fractures of the nasal bones; nasal trauma can also mean that you have trauma to the cartilage of the nose or soft tissue trauma. Sometimes these are non-operative.
Minimally or non-displaced fractures can usually be managed with close observation.
Indications for surgical repair (when there is obvious displacement, like the nose is crooked) are lateral displacement of one or more nasal bones, comminuted or depressed nasal bone fragments, or frank impaction of the nasal pyramid.
Nasal Fracture Reduction
This procedure can be performed in the OR or in clinic, depending on patient and surgeon preference. The goal is to shift the nasal bones into their native position. It is not a great option for trauma to the nasal cartilages, mainly if there is a nasal bone fracture. It should be performed within two weeks, before the bones heal into their new position.
Case Example: Nasal Fracture
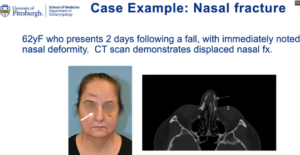
A 62-year-old female presented two days following a fall with immediately noticed nasal deformity. A CT scan demonstrated a displaced nasal fracture.

The patient was a good sport, and her injury was taken care of in the office. Dr. Yver reduced the bones back into their proper position during a 10-minute procedure. Fortunately, when the patient came in for follow-up and the cast was off, she had excellent realignment of her nasal bones and the external deformity was corrected. This was a straightforward nasal fracture. Another patient had a much more severe nasal trauma.
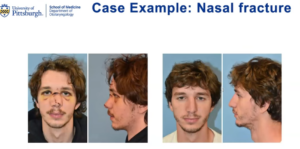
Case Example: (More Severe) Nasal Trauma

A 21-year-old professional male hockey player took a hockey puck to the face. His nasal bones were completely shattered and impacted, and he could not breathe at all through his nose. This absolutely something to address in the acute period because it would not be easily addressed in a delayed fashion. He went to the OR because Dr. Yver wanted to have the best possible set up. She remolded his nasal bones, which fortunately were all very mobile. His nose was packed and an external splint was fashioned to hold everything together.
Four months later, the patient returned to see Dr. Yver. “I love when my patients come back to see me because we were able to appreciate that he just has this excellent restoration of his dorsal height,” she said. “He looks like nothing ever happened to him. He’s breathing great. This was a success story.”
In fact, the patient flew in from Vermont because his insurance would only cover care in PA. Every time he had to see Dr. Yver, he had to get on a flight.
Nasal trauma can also involve the soft tissue of the nose, which can be a real problem.
Case Example: Nasal Soft Tissue Trauma
A 33-year-old avid mountain biker went over his handlebars while wearing sunglasses. The sunglasses were pushed down his nasal dorsum, resulting in the soft tissue fragment hanging on by one little skin bridge. One of the “fantastic” residents saw him in the ER and sewed him up right then and there.
Dr. Yver was worried about him because the soft tissue was very purple and congested. She was concerned that its blood supply might have been so disrupted that it would not survive. But when she saw him a week later, it was clearly a viable soft tissue. Four months later, he had a scar, but only if you looked hard to see it. He was still wearing sunglasses, unfortunately, but this was another great success story and “great work by one of our residents.”
Panfacial Trauma
Multiple facial fractures can result from high-velocity impact (e.g. ATV accidents, motor vehicle accidents, fall from significant height). A Lefort fracture is defined by a fracture line involving the pterygoid plate. This was named after a French surgeon named Renee Lefort who studied craniofacial trauma in the early 20th century. The story goes that he took cadaver heads and threw them repeatedly at a wall and then dissected them to observe common fracture patterns. He found there were predictable patterns of fractures and three common patterns of midface fracture that directly involved the pytergoid plate. This came to be known as Lefort one, two, and three fractures.
Since these are high-velocity injuries, these patients often have other things going on. They have significant intracranial imaging injury. They might have spinal trauma. They are often seen in the ICU, where repairs are done on an impatient basis.
Case Example: Panfacial Trauma
A 65-year-old man was on his deck on a very windy day. The wind blew over his large patio umbrella, and the tip of the umbrella struck him in the right cheek and went through his sinuses through the inside of his nose. It displaced a huge fracture next to his left eye essentially into his left orbit.
The patient was in really bad shape when he presented to one of the Level One Trauma Centers. While this was an unfortunate injury, it was a miracle that the umbrella did not go posteriorly into his skull base or intracranially.
When Dr. Yver was reviewing the CT images with one of the residents, the resident pointed out some heterogeneous material in the left maxillary sinus. Dr. Yver did not think too much of it, thinking it was a hematoma or debris. She figured they would see during surgery. Two days later when the patient was taken to the OR, they started with a nasal endoscopy. The first thing Dr. Yver saw was a little bit of foreign material peeking out. A sinus instrument was used to pull it out. It was a big piece of fabric from the umbrella that had somehow gotten sheared off and lodged into the man’s sinuses.
Once the foreign bodies were removed, it was still an almost six-hour operation. All the fractures around the orbit had to be exposed and the plates added. He had a huge orbital floor defect, so that had to be plated. He also had nasal trauma, so his nasal bones had to be reset. Full sinus surgery was done to clean out his sinuses where they had just been obliterated from the blunt trauma. Then ocuplastics and a strobisma surgeon joined the team because there was some damage to his extraocular muscles, which had to be repaired directly by ophthalmology colleagues.
Upon post-surgery imaging, there was excellent reduction of all the displaced bony fragments. Several plates were in place, sitting exactly how they were supposed to. The patient did well postoperatively and was discharged after two days in the hospital.
Logistical Challenges
Increasingly, fewer providers manage operative facial trauma in the community, which means patients may need to be transferred to a tertiary trauma center. Patients can come from really far away, so not only is this a problem for their evaluation and getting them scheduled for surgery, especially if done on an outpatient basis, but it is also hard for follow up and reliable check ins after surgery.
This patient population tends to be underinsured, further limiting access. Dr. Yver said this is really frustrating, as they have patients who present to the ED with acute trauma that is operative. Even though they need surgery, they are discharged. It turns out that even though they were brought to this ED, their insurance does not cover UPMC to do their surgery on an outpatient basis. So they have to find someone else to do it, somewhere like Ohio. It can be really hard to find a surgeon who does this type of surgery, especially if the patient was not evaluated in that ED. “We try to help these patients as much as we can to get the care they need, but sometimes we’re just limited by the system,” Dr. Yver said.
Add on cases are subject to OR availability and staffing. These cases are time-sensitive and relatively acute, so they often have to happen on an add on basis. The OR is limited as it is in terms of capacity, so surgeons like Dr. Yver are subject to OR availability, whether the staff is there to accommodate. And that is not the only obstacle. “You never know if something more acute’s going to come in the door, like a brain bleed,” Dr. Yver said. “Getting these cases in and done is always a logistical challenge.”
Patients are often lost to follow up despite best efforts. This has been a focus of a lot of research efforts of the facial trauma group. The idea is that they are trying to identify some reliable predictors of patients who are at high risk of being lost to follow up after their trauma is treated. Interestingly, what they found by looking at their own data is that patients who have surgery on an impatient basis, discharged without having their follow up appointment already scheduled, and those who come from regions with a relatively high area deprivation index tend to be lost to follow up after surgery.
“What we’re trying to do is use this information to identify these patients in advance and then come up with the strategy to ensure that they have reliable access to care long-term even after their surgery, so we can be available if there are complications, concerns, or issues,” Dr. Yver said. They are also using this information for their own learning and research.
Dr. Yver really enjoys facial trauma as part of her practice, and said it is extremely rewarding. “We make a huge difference in the lives of our patients, some of whom have been through some really traumatizing events,” she said. “But there are still a lot of logistical challenges associated with managing facial trauma.”