How important is precision survivorship and why does it matter? These questions were posed by Marci Nilsen, PhD, RN, CHPN, FAAN, Co-Leader of the Cancer Risk, Outcomes and Preventions Program at UPMC Hillman Cancer Center, and Director of the UPMC Head & Neck Cancer Survivorship Clinic in the Eye & Ear Foundation’s March 24th webinar, “Precision Survivorship: Using Data to Transform Care.” Assistant Professor Kevin Contrera, MD, MPH, also presented, focusing on precision surveillance and response – adapted treatment.
Survivorship Care Lagging
New data about cancer survivorship found that a lot of patients are being cured and living longer. To this point, Dr. Nilsen said that survivorship is not just a short phase for most patients; it will become the reality for much of their cancer care experience. In fact, Dr. Nilsen said, “We are curing more head and neck cancer (HNC) than ever, but survivorship care hasn’t kept pace.” Additionally, HNC incidence is rising, and survivors carry some of the greatest treatment side effects of any cancer population – making precision survivorship more urgent than ever. Immunotherapy is becoming increasingly common. This matters because “this is really how we can ensure that patients are not just surviving but living well after we cure them,” Dr. Nilsen said.
Survival is just the beginning. Multiple studies have looked at what patients report. To illustrate what survivors experience, Dr. Nilsen created a word cloud capturing the most commonly reported treatment-related effects across these studies.

A large study out of Norway showed that about 83% of patients have at least one treatment-related effect. Common ones are fatigue, neuropathic pain, and sleep disturbances.
What do patients at UPMC report and how common are these issues? In her work on this patient population, Dr. Nilsen found that 56% of HNC survivors report three or more treatment side effects while 90% of patients report at least one, most commonly trouble swallowing, dry mouth, and pain. These are side effects they report as being important to them and ones they deal with daily.
Precision Survivorship
“How can we work collaboratively to be able to better treat and help patients survive beyond their cancer diagnosis and really live beyond that?” Dr. Nilsen asked.
The answer: precision survivorship.
“We’ve taken the data; we know what patients report,” Dr. Nilsen said. “We know some of the most significant issues they have, and we’ve really built a team that allows us to provide tailored care to patients at any point in their survivorship journey.”
Three tiers define this approach:
Identify: Systematically screen survivors for unmet needs
Intervene: Connect patients with targeted rehabilitation services, education, and support
Improve: Use data to continuously learn and refine care
Integrating Survivorship
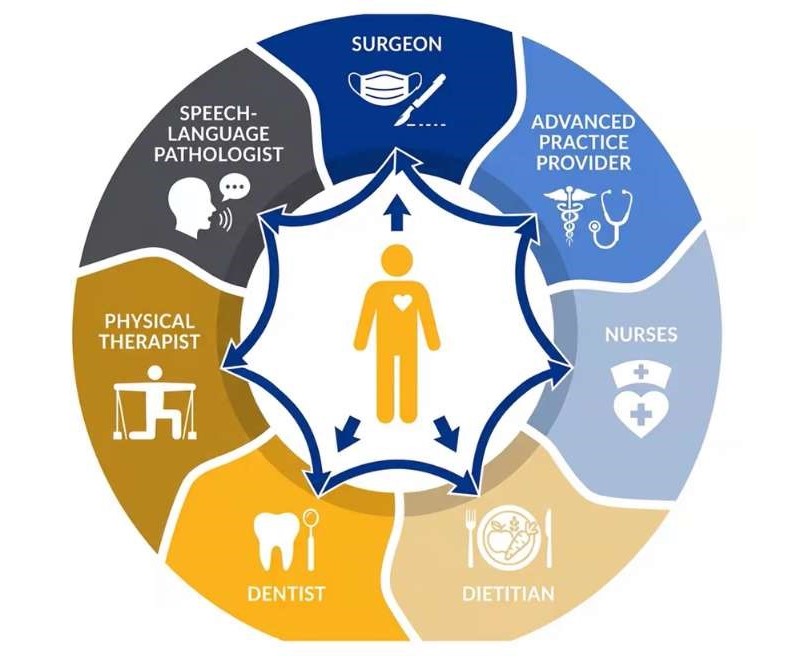
The issues that patients experience are vast and generally not best addressed by one provider. The multidisciplinary team is built around patients, consisting of nurses, a speech-language pathologist, Advance Practice Provider, dentist, dietician, and physical therapist. The dietician, for example, helps patients get the right number of calories. Radiation can damage teeth no matter how diligently patients care for them, so the Clinic connects patients with a dentist early on to offer guidance and support along the way.
“Survivorship focused on the health and well-being of a person with cancer from the time of diagnosis through their entire life,” Dr. Nilsen said. “This should be something that is really integrated into every step of the process.”
Family members, friends, and caregivers are also considered part of the survivorship experience. They may experience the journey in a different way, but it is important to help them – not just for their health, but the survivor’s health.
Moving Forward
How is the Survivorship Clinic taking the data and moving forward? Research has shown that earlier care results in better outcomes: better quality of life – physically and emotionally, a year after treatment, less depression and anxiety, and less difficulty swallowing, sleeping, and neck pain.
A medical student in the Clinic looked at patients who came after radiation versus patients who were integrated before radiation. When matched on the key variables that might impact their outcomes, patients who came to survivorship early prior to radiation had better quality of life. They had a lot fewer symptoms than the patients who came after.
This is important because it shifts “our paradigm of thinking, of intervening after radiation,” Dr. Nilsen said. “I also think it challenges the national stage that we have. Much of survivorship care in the accreditation standards don’t recommend or require survivorship services until after treatment.”
Despite patients who visited the Survivorship Clinic before radiation doing measurably better – in body and mind a year later – not everyone gets this kind of care. Only half of HNC patients attended the Survivorship Clinic within five years of diagnosis. Patients living further away were less likely to come; those living more than 60 miles away were about half as likely to attend. Patients with more advanced cancers were also less likely to attend. These findings were published in the Journal of Cancer Survivorship in 2025 (Owoc, Carlson & Nilsen).
“If earlier care leads to better outcomes, we have to make sure everyone can access it,” Dr. Nilsen said. So, how can more survivors be reached?
- Navigation: Helping patients find and access care
- Multiple modes of care: Collaborative clinic, surveillance visits, and telehealth
- Engaging clinicians: Making sure the providers who see these patients first know to refer them and what survivorship care looks like
“We’re not waiting for survivors to find us; we’re meeting them where they are,” Dr. Nilsen said.
Breaking News
Starting in February, in addition to the collaborative clinic (on Thursdays), a more streamlined clinic is available for patients with less symptoms than some of the more complex patients. Telehealth and telemedicine are being rolled out, allowing the Clinic to potentially reach patients who are frail or might not be coming in person due to travel time. “Navigation becomes very important because we want to make sure we can get these patients we see on telemedicine into services that will benefit them,” Dr. Nilsen said.
The Clinic is constantly working with clinicians on clinician engagement. “We try very hard to ensure that we identify patients who could benefit,” Dr. Nilsen said, “and we collaborate with not just our clinicians here but ones in the community. You can come whenever you want to come – preferably before – but we will see you at any point.”
Current Research
So far, what Dr. Nilsen discussed focused on changing models of care, changing real-time what the Clinic focuses on, how the Clinic delivers care, and how they advocate for these approaches to become standard. But there are other aspects to what they do, such as attempting to answer questions like, what does our data tell us? Why do some survivors struggle more than others? Can we predict who is at the highest risk before problems get worse? Can we find biological clues in the blood that tell us what’s coming?
As a clinician, Dr. Nilsen said sometimes she can read about two different patients in a paper who sound very similar – similar age and treatment – but when she walks into the room, they look different. Ideally, the data would answer the aforementioned questions.
The Clinic is trying to work on topics that are the most pressing to its patients. So, what matters to them? Swallowing, saliva, and pain – these are not just side effects. They are what define daily life after treatment. Pain is a significant effect that patients experience, which has not changed since 2016 when Dr. Nilsen first started looking at this data. It is still what patients report in their top five issues. Trying to better understand this has led to a couple of different projects.
“Neck patients are common and they matter,” Dr. Nilsen said. About half of the Clinic’s patients have some degree of neck pain or neck problems. Generally, this refers to pain with movements and daily activities, pain in the neck that stops patients from doing the things they love and can contribute to a worse quality of life. Half of the Clinic’s patients report some degree of neck disability, and the patients who report some degree of neck pain are more likely to have lower social and physical quality of life. If a patient just has surgery, they are less likely to experience this. If a patient has chemo and radiation, they are more likely. Surgery plus adjuvant treatment or surgery plus chemo and radiation, they are more likely to have side effects in their neck. There is no real difference between a non-operative group and surgery plus non-operative, or plus chemo and radiation.
“That’s why we’ve always focused or increased focused on seeing patients pre-radiation, because that seems to be a common denominator in some symptoms we see,” Dr. Nilsen said.
Research done by a UPMC resident several years ago found that neck and swallowing problems go hand in hand. They share the same root, which means that treating one may help the other.
Predicting who will struggle before it happens is another area of research. Some patients get better over time, but some do not. “We’re learning to tell the difference early,” Dr. Nilsen said. Patients are being tracked from before radiation through two years after to understand how these problems develop. Not everyone follows the same path. Some people start out worse while others stay steady. There is a middle group that is a little unique – they start out having symptoms, get better, and then the symptoms worsen. Advanced treatment stage or advanced tumor stage can contribute, along with other characteristics like not being married (which relates to social support and integration into services). Knowing these characteristics beforehand may give providers an idea of who to target with more tailored approaches.
Dr. Nilsen is also looking at biological markers in the blood that may predict who is at highest risk. She believes that radiation-induced fibrosis is a contributing factor. This is the tightening of the skin and underlying muscle that limits movement of the neck in multiple different directions. It affects strength, endurance, and contributes to spasms and pain and can limit function.
The good news is blood markers may predict fibrosis. The team found specific biological signals in the blood that were present in patients who developed the worst scarring after radiation. MicroRNAs control which genes get turned on or off in the cells. When radiation damages tissue, certain microRNAs shift, and these shifts can trigger the scarring process. These same signals appeared in patients and animal models exposed to radiation, suggesting they are real and reliable markers. These markers are linked to the body’s scarring and inflammation pathways, meaning they may tell us why some patients develop severe fibrosis and some do not.
FOCUS: Ongoing Research
Some survivors do much worse than others, and it is not fully understood why. Dr. Nilsen believes these differences follow predictable patterns, and that they can identify who is at highest risk early. They are looking at lifestyle, treatment, and blood markers to build a complete picture of who needs the most intensive care. “This NCI-funded research is happening right here in Pittsburgh, with our patients, for our patients,” Dr. Nilsen said.
Precision Surveillance and Response – Adapted Treatment
Dr. Contrera’s presentation focused on one sliver of survivorship: surveillance. In a similar vein to what Dr. Nilsen covered, Dr. Contrera discussed using data to guide treatment therapies in a way that is personalized to the individual based off their own biomarkers. His research is a combination of three different things. He came to Pitt very interested in building clinical trials and at the same time wanting to personalize therapy through response-adapted treatment, “which is to say that we’re modifying cancer treatments real-time based on our assessment of disease,” he said.
Disease can be assessed with biomarkers. Dr. Contrera’s particular interest is in using a type of liquid biomarker called circulating tumor DNA, or ctDNA.
Patterns of Recurrence
How do we know if and when patients are going to recur? Dr. Contrera’s colleague Kate Herring, MD, looked at patterns of recurrence. If patients recur, almost half will have recurred within six months, with 75% by a year. The vast majority (80%+) will recur within two years. “This is the window in which we’re focusing on the identification of these recurrences so that we can either treat them, or even better, can we prevent them?” Dr. Contrera said.
The patients who did worse were those who were HPV-, had a high neutrophil/lymphocyte ratio, or poor performance status (drinkers and smokers – three times more likely to recur). Cyotoxic CD8 + T lymphocytes are responsible for killing cancer cells. They have been shown to predict outcomes and response to treatment in various malignancies. However, HNC lags behind many other fields in the standardized use of this biomarker.
What does this mean in terms of a patient’s likelihood of survival? When looking at different studies, patients with a high number of infiltrating lymphocytes are far less likely to recur because that means the body is seeing the cancer as foreign and attacking it. This can be anywhere from a 20% less likelihood of recurrence to 60-70% for oropharyngeal cancer. When looking at overall survival, the effect size is just as large.
If using this ratio in patients who underwent surgery, they are 10 times more likely to recur, which makes it a better biomarker than any of the standard things like staging or smoking.
Identifying recurrence is more than just predicting who is and is not going to recur. “I want to try to push us even further into actually identifying recurrences earlier,” Dr. Contrera said.
Circulating Tumor DNA
One way to do this is to look at ctDNA. Circulating tumor cells are individual tumor cells found in the bloodstream that have been described as the seeds of dissemination and metastasis. During tumor apoptosis or necrosis, tumor cells release their genetic materials into the bloodstream, which is called circulating tumor DNA. ctDNA tends to have a high sensitivity and is a promising tool for prognosis and detection of disease/recurrence.
In a meta-analysis – where a bunch of studies are brought together to figure out the benefit – of patients with HNC, patients with detectable ctDNA in their blood are sevenfold more likely to recur. The numbers are more striking when looking at overall survival. What was shown for the first time was if ctDNA is in the bloodstream, the patient is tenfold more likely to die of any cause. “This tells us it is a very good biomarker,” Dr. Contrera said, “beyond just predicting who is going to recur and when. The most important thing we can do for patients is to move this into a therapeutic paradigm, meaning, can we actually use this data real time to impact patients’ treatments?”
This is where clinical trials come into play.
LymphDetect
LymphDetect significantly stratifies recurrence risk in intermediate risk HPV- HNSCC. These patients do not do very well as half will recur within two years. If looking at the ctDNA not in the blood, but in the drain fluid (work pioneered by José P. Zevallos, MD, MPH, FACS, Chair of the Department of Otolaryngology-Head & Neck Surgery and a close mentor of Dr. Contrera), it can be determined which patients will do well.
In patients who do not have detectable ctDNA in their drains, only about 10% of them will recur. If their ctDNA is detectable, the vast majority (2/3) will recur. The separation is quite striking, even at a year out.
LymphDetect also significantly stratifies recurrence risk in intermediate risk HPV- HNSCC patients who have only received radiation treatment. Not a single patient recurred if the ctDNA was negative, while the majority of patients with positive ctDNA recur. This data is being collected right after surgery before getting standard radiation or chemo, which is a critical time before receiving treatment.
Dr. Contrera is leading a multi-institutional trial at five different centers across the U.S. which is utilizing this ctDNA drain fluid to guide therapy. Patients in the intermediate risk category after surgery will get standard radiation if the drain fluid is negative. In a subsequent trial, the goal will reduce the amount of radiation given to these patients since these patients do so well.
If the drain fluid is positive, in addition to radiation, these patients will receive chemo. “What we suspect is that by titrating the adjuvant therapy based off the risk, we will be able to significantly decrease the number of patients that recur,” Dr. Contrera said. This will be one of the first trials in the country using this liquid biomarker to guide therapy, and one of the first in HNC. “We are really pioneering in this space to try to personalize therapy through these different liquid biomarkers,” he added.