Dedicated cancer epidemiologist Angela L. Mazul, PhD, MPH, who specializes in head and neck and HPV-associated cancers, explained that her job is studying risk factors and trends in the Eye & Ear Foundation’s April 30th webinar, “Incidence and Prevalence of HPV-Related Head & Neck Cancer.” Her role is important because HPV-related oropharyngeal cancer (OPC) has been rising dramatically.
What is the Oropharynx?
The oral cavity is in the front, and includes the lips, front of the tongue, and mouth. The oropharynx is behind that and refers to the throat, which includes the soft palate in the back, the back wall of the throat, tonsils, and the back part/base of the tongue.
These tissues have lymphoid cells, which are also immune cells that can be infected by HPV. This accounts for about 60-70% of OPCs. Patients with OPC present with a persistent sore throat, difficulty swallowing, ear pain, and most commonly, with a neck lump.
Early detection is hard with this cancer because symptoms can be mild at first. Unlike cervical cancer, there is currently no standardized screening test for HPV-related throat cancer because of where the cancer develops; it is difficult to reach.
“Awareness and prevention or vaccination is key for this cancer,” Dr. Mazul said.
Why it Matters: Rising Throat Cancer
Incidence of OPC is rising rapidly, especially in men, due to HPV infections. OPC is now the most common HPV-related cancer.
“It is one of the biggest shifts in head and neck cancer (HNC) in the US,” Dr. Mazul said. Historically, most of these cancers were driven by alcohol and smoking. As smoking rates have declined, these cancers have as well. At the same time, however, HPV has caused a dramatic rise in HNC, specifically OPC. Since the mid-2000s, incidence has risen by 1-2% a year.
Most oropharyngeal cancers diagnosed today in the United States are HPV-associated, which has surpassed cervical cancer as the most common HPV cancer in the US, with roughly 22,000 new cases each year.
This is particularly concerning because it is reflected in mortality trends. After years and years of decline in the number of people who are dying with HNC, it has begun to rise again. This represents a reversal of prior trends in head and neck cancer.
“The important takeaway here is this is preventable,” Dr. Mazul said.
Traditional Risk Factors
Before HPV, throat cancer mainly came from heavy smoking and/or drinking. If you do both heavily, you have an almost 30-fold higher risk of developing HNC compared to those who do neither. If you smoke, you’re 11 times more likely to get cancer. If you just drink, you’re twice as likely.
Smoking still plays a role in who gets cancer. It is measured by cumulative tobacco exposure, called pack years. If you smoke a pack a day for a year, that equals one pack year. Both the time and number of packs you smoke are cumulative.
What is HPV?
Human papillomavirus is an extremely common virus that has evolved with humans. The cells lining the cervix and the oropharynx share biologic similarities that make them susceptible to HPV infection. Most adults are exposed to HPV at some point in their lives. There are over 100 types. About 40 of those will infect the mouth, throat, or genital areas, and they typically spread through intimate skin-to-skin contact.
Most HPV infections do not cause any problems and will clear on their own. Our immune system has evolved with us, so our immune system can fight it and clears most of them. It is when infections persist over time that drives cancer risk.
Not all HPVs are the same. They are classified into two groups: low-risk and high-risk. The low-risk groups are the ones that cause warts on the fingers, hands, or genitals. High-risk types are the ones that cause cancer, especially HPV 16, which is responsible for the vast majority of OPC cases. Other high-risk types, like 18, 31, and 33, also contribute but are less common.
The HPV vaccination covers nine types, including the most common ones that cause OPC.
Time From Infection to Cancer
OPC does not develop overnight; it develops over a very long period of time. Viral infection happens first, and this is where it stops for most people. But sometimes the virus persists and causes changes in the cells. Those infected cells then grow and divide abnormally, and over time, accumulate genetic changes progressing from normal tissue to pre-cancer, and then invasive cancer. The span can be as long as 30 years.
Hopefully one day there will be a screening tool so it can be caught earlier.
How Common in the US?
In the US, HPV-associated cancers are pretty common. Annually, there are about 50,000 cancers diagnosed in areas where HPV is found, and 80% are caused by HPV infection. For women, cervical cancer is still the most common HPV-related cancer, though rates have been declining because of screening.
For men, however, OPC is now the most common HPV-associated cancer – more common than any other cancer. There are about 22,000-23,000 cases of OPC a year.
Worldwide Distribution
HPV-related OPC is most common in high-income countries, like Europe, Australia, and the US. Lower-income countries have lower diagnosed cases yet higher rates of smoking. About 30% of all OPC worldwide are HPV-driven, and many developing countries are seeing increased trends of HPV-associated cancers. Sixty-three percent of all countries have committed to WHO vaccination programs, though only 34% of them are gender neutral. The rest are only vaccinating women.
“Globally, there should be a push to vaccinate both men and women,” Dr. Mazul said.
Increasing Epidemiology of OPC
While HPV OPC has increased dramatically over the past several decades (almost 200%), there are differences between race and gender. White men have seen a meteoric rise. Among Black men, it is decreasing, while it is increasing among Hispanic and other races.
Women have similar trends, but at a much lower rate. Smoking-related cancers are going down, so HPV is coming up as a risk factor, which could be a replacement effect.
Men have a 4-5-fold higher incidence of OPC than women. It is primarily a disease of middle-aged adults, as the average age of diagnosis is 63. For HPV- cancer, it’s a little older, around 68.
HPV-Positive vs HPV-Negative
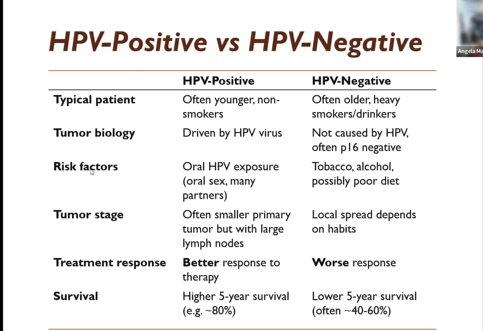
The two are markedly different. HPV status is the strongest prognostic factor of OPC, which is why the staging system has now separated positive from negative. Your clinician should test for HPV if you have OPC as HPV+ or -.
Although outcomes are often favorable, treatment can still be physically challenging. There are a lot of clinical trials trying to make it more bearable because survival is so good.
How HPV Gets Into Your Throat
Dr. Mazul called this the elephant in the room. The root cause of this cancer is oral HPV infection, and the most important risk factor is simply exposure to the virus. It is not about a single event but having multiple/cumulative exposure.
Oral HPV infection is associated with oral sexual exposure, particularly with greater lifetime numbers of oral sex partners. The younger someone is, the more the number of partners increases, not only oral HPV but oral HPV prevalence but also the risk.
A study conducted in the UK found gender differences. One of the hypotheses is that men have a higher risk or higher HPV oral prevalence compared to women due to differences in exposure, as men have more oral sex partners than women.
There is also a hypothesis that women are more likely to transmit HPV to men. Another theory is that HPV has been affecting the cervixes for a long time, so maybe women are better at clearing oral HPV compared to men.
The immune system plays an important role, so if it is weakened, the body is less able to clear HPV.
In Dr. Mazul’s work, looking at U.S. veterans, individuals living with HIV had about a 70% higher risk of oropharyngeal cancer compared with HIV-negative veterans
Traditional risk factors like smoking or alcohol use still matter.
Hidden Tumors
Where these cancers go are in places full of crypts and hard to get to, which is why they are difficult to see. The primary tumor is extremely small, typically does not cause pain, and has no obvious signs. Patients often notice a neck mass, or something just feels off, long after the initial growth has started. Because these patients often lack classic risk factors, patients and doctors don’t really suspect cancer first. Patients have a tendency to get bumped around to different specialists first before coming to ENT and getting a diagnosis of cancer quickly. In many HPV+ cases, they’re diagnosed when they spread to the lymph nodes.
Dr. Mazul is also a disparities epidemiologist, which has a lot to do with access to care. If you have access to high quality care and see the right person first, you’ll get diagnosed sooner. But if your PCP doesn’t know what’s going on or doesn’t know about oral HPV being associated with OPC, it might take a while for you to get from your PCP to an ENT who can diagnose things. Access to care becomes very important with these cancers.
Good News for HPV-Positive Cancer
The good news is that HPV+ OPC have much better outcomes. One study found that only 10% of patients died within two years vs 33% of HPV- patients. A 2010 paper in the New England Journal of Medicine was the first one to show this. It found a 5-year survival rate at 80% or more for HPV+ and 40-60% for HPV-, even when stages are similar. “We think this is because HPV tumors respond better to chemoradiation than traditional HPV- tumors, and they’re inherently less aggressive,” Dr. Mazul explained.
This still means 10-20% of patients are dying and not getting to a cure, making early detection and prevention still very important.
One of the first studies Dr. Mazul did found that patients with the HPV 16 subtype had much better survival than those without. This has been replicated many times, and people in the genomic space have been investigating why this is the case.
Not only are there differences between HPV positive and negative, but also within HPV+. The type of HPV you are infected with matters.
Traditional Risk Factors Still Matter for Survival
People with heavy tobacco use – especially those with 10-20 pack years – have substantially worse outcomes. If you quit smoking or drinking during treatment, you do a lot better.
Testing the Tumor
The first thing your doctor should do is a P16 test, an immunohistochemistry test that targets P16, which is downstream from HPV. HPV infects the cell, which upregulates P16.
The new staging system for HPV testing could guide treatment and prognosis. There was no hard rule for testing HPV until 2018.
Disparities: HPV Testing
Prior to the 2018 guidelines about testing, there were disparities in who was being tested. Patients with Medicaid or no insurance were significantly more likely not to be tested. Patients with Medicaid were 80% more likely to not be tested, and uninsured were 75% more likely not to be tested compared to people who are privately insured. Testing rates were also lower in low volume and non-academic centers as well.
There were also racial disparities, with Black patients less likely to be tested. Disparities by income still exist, with those in lower-income brackets having a lower test rate.
Since 2018, the numbers have improved to somewhere in the 90% range, but Dr. Mazul wants to see this as close to 100% as possible. “At least, the people who are not insured should be just as high as people who have insurance, to make sure everyone has equitable treatment,” she said.
Prevention: HPV Vaccination
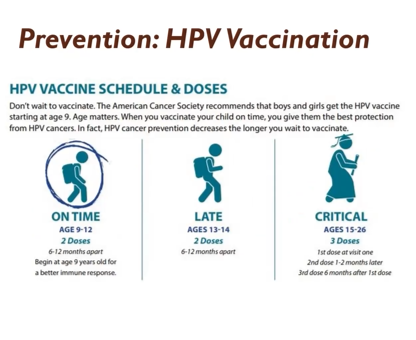
The best time for the best immune response is nine years old, before any risk of sexual encounters. Vaccination is now available for both genders.
Dr. Mazul recently got a grant funded to ascertain whether it is cost effective to look at HPV vaccination in veterans since their risk of OPC is much higher compared to the general population. Is it worth extending their vaccination past 26 to 45?
In veterans aged 18-26, only about 30% of women and less than 20% of men have started the HPV vaccination series. Clear patterns were seen when Dr. Mazul investigated this; women were more likely to get vaccinated than men, and young people were more likely compared to older ones. This is in a population that already has an elevated cancer risk.
“This is a really big, missed opportunity, especially in veterans,” Dr. Mazul said. They already have their healthcare covered by the government, so it costs nothing out of pocket to get vaccinated.
Unfortunately, this is not just limited to veterans. Dr. Mazul looked at the UPMC healthcare system, and only a third of women and a quarter of men had completed the full vaccination. There are a lot of disparities. Lower socioeconomic status groups are more likely to start the vaccine but less likely to complete it.
Some studies suggest fewer doses may still provide protection, but current recommendations still support completing the full vaccine series. In older patients, three is the goal.
In addition to barriers to care and access, stigma around HPV as a sexually transmitted infection is an issue. Even though the vaccine is safe and effective, people are not receiving it.
Effect of Vaccination (Future)
A modeling study done by a colleague of Dr. Mazul shows that even with the current vaccination rates – in which the curve has bent a little bit – rates are expected to rise through 2030.
His study found that 54% of adolescents and 21% of young adults received the recommended dosage.
The good news is around 100,000 cases a year are lost due to vaccination – that is a lot of people not getting cancer.
Life After Cancer
Even though HPV-related throat cancer is survivable, survival is not the whole story. For many patients, treatment can lead to long-term effects. This includes difficulty swallowing, changes in taste, dry mouth, and speech. Pain is a big one, depending on the type and intensity of treatment.
After patient treatment ends, there are still many challenges and ongoing daily life. That is why survivorship care is really important. The team approach means that you see many specialists in follow up speech and swallowing therapies, nutrition specialists, dental providers, and very often, mental health support. The goal is to maintain quality of life.
Since patients are younger, this leads to other considerations. If diagnosed at the average age of 63, this is before many retire. People are having kids at older ages, so maybe you have kids who are not out of school yet.
Therefore, it is important to understand that while you are likely to survive your cancer, being aware of what happens in the survivorship period is crucial to help maintain quality of life. Dr. Mazul read somewhere that right now there are about half a million HPV+ OPC survivors – that is a lot. This number is just going to increase.
Takeaways
- HPV-related throat cancer is increasing
- It affects more men than women
- Treatment impacts quality of life
- Vaccination can prevent it
“Vaccinate early and vaccinate often,” Dr. Mazul said. ”Often, in that you should make sure to get your two doses or three doses depending on when you get vaccinated.”